Public transit is one of the safest indoor spaces during the COVID-19 pandemic for a plethora of reasons. But the perception of transit’s safety is lagging. The Centers for Disease Control and Prevention (CDC) has a lot of power to change the narrative and pursue vaccination sites that are transit-accessible, as we wrote in a joint letter to the agency with our partners.
New York MTA’s Mask Force distributing free masks to subway riders. Photo courtesy of the MTA.
Public transit is incredibly important to our pandemic response, connecting riders and essential workers to jobs, groceries, healthcare and more—safely. With proper precautions such as wearing a mask, transit is one of the safest indoor spaces for COVID-19 transmission, with a plethora of studies failing to link disease spread to transit.
Why is transit so safe? Buses and trains are highly-ventilated; riders must wear masks (thanks to a new requirement from the CDC); vehicles are cleaned frequently; and riders tend to spend a short amount of time on vehicles and in stations.
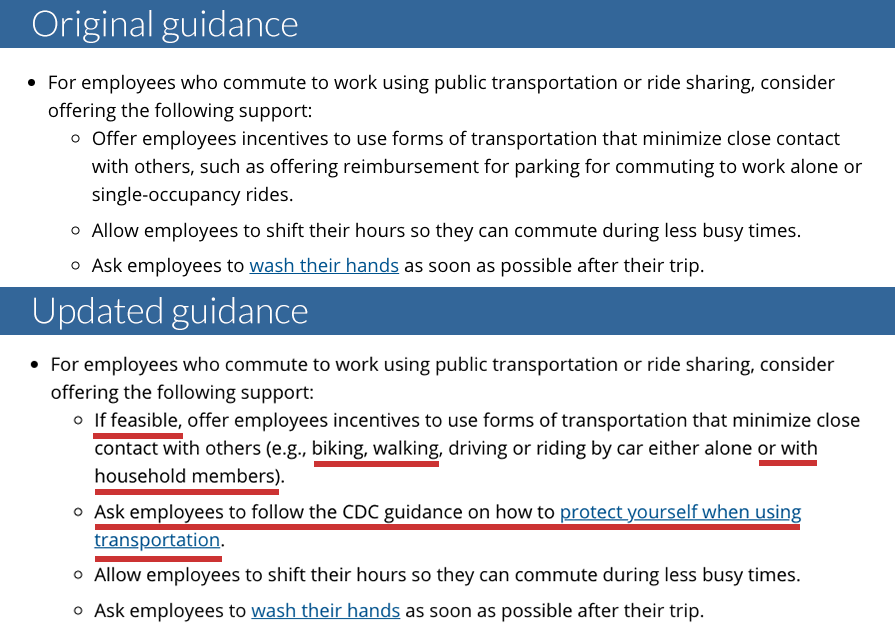
But the CDC isn’t clearly communicating transit’s safety to the public. In fact, last summer the CDC actively encouraged Americans to avoid transit—guidance they updated after criticism from Transportation for America and our partners.
While we’re grateful that the CDC updated this guidance and last month instituted a mask requirement on transit and other forms of transportation, the CDC needs to do more. CDC guidance that does not make it clear that transit is safe undermines public confidence in this essential service and ultimately undermines our communities today and our recovery tomorrow.
We urged the new CDC director, Rochelle Walensky, to communicate transit’s safety in a new letter written by Transportation for America and signed by our partners the Transport Workers Union, TransitCenter, the American Public Transportation Association (APTA), and the National Association of City Transportation Officials (NACTO). You can read the full letter here.
It is also critical that the CDC considers transit access as a determining factor in choosing vaccination locations, and to provide guidance to states to ensure no one is denied access to a vaccine. As we wrote in our letter, no one should be denied access to a vaccine because they do not have access to a car. Public transit can and must play an important role in providing Americans with safe, convenient, and equitable transportation to vaccination appointments.
We urge the CDC to clearly communicate how safe transit is to the public, and make transit access a factor in determining vaccination sites. Americans need transit—the CDC shouldn’t undermine it.